General medicine case-2
This is an online E log platform to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. I have been given this case in order to solve in an attempt to understand the topic of patient's clinical data analysis to develop my competency in reading and comprehending clinical data and come up with a diagnosis and treatment plan.
Introduction
-50y old female came to casuality with complaints of fever since 8 days, which is high grade,associated with chills,generalised body pains,headache and is realived on medication.
-Cough since 8days ,non-productive and not associated with sob.
-No h/o hematuria, rashes on the body
-No h/o burning micturition.
HISTORY OF PAST ILLNESS
K/c/o Dm and patient is on tab.glimiperide 1mg
Tab.metformin 500mg
Not k/c/o HTN, TB, asthma, epilepsy
TREATMENT HISTORY
• Not k/c/o HT, CAD , TB.
•NO H/O chemo /radiation , blood transfusion.
•NO H/O previous surgeries.
FAMILY HISTORY
-Not significant
VITALS
Temp: 98.8
PR: 78bpm
BP: 120/90mm hg
RR: 18cpm
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
CVS: s1s2 heard
•No murmurs
RESPIRATORY SYSTEM:
•NVBS heard
•Position of trachea - central
•Breath sounds - vesicular
RS: BAE+ NVBS+
ABDOMEN
P/A: soft, non tender, bowels sounds heard
CENTRAL NERVOUS SYSTEM:
•Intact
•No focal defect
CNS: NFND
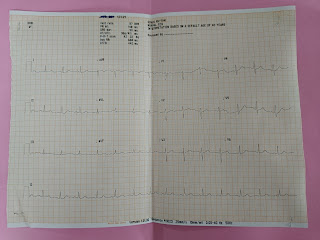
INVESTIGATIONS
HB: 10.2
Platelets: 2.39lakhs /cu mm
CUE: alb +
S creatime_0.9



Provisional diagnosis:
-Viral pyrexia ? Secondary to dengue IgM positive



Comments
Post a Comment